

Introduction
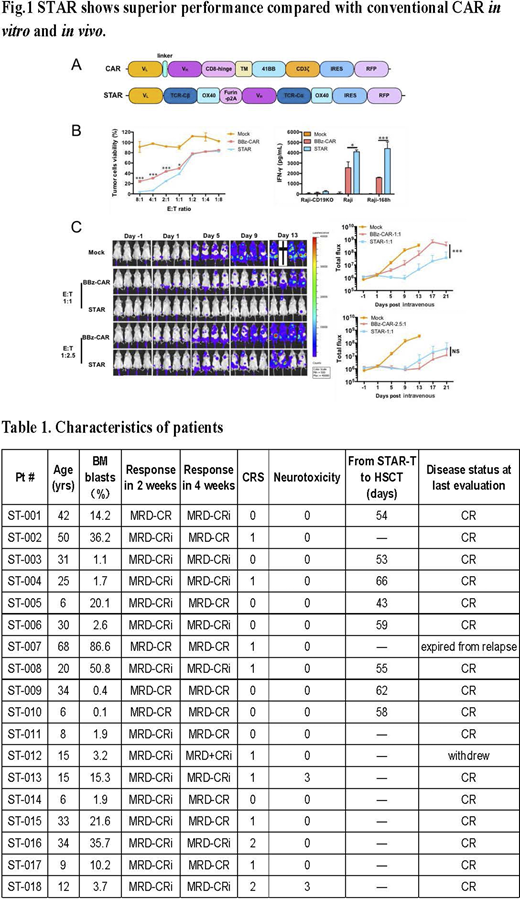
Chimeric antigen receptor (CAR) T -cell therapy has demonstrated high response rates among patients with B cell malignancies yet remission durability and safety could be improved. We have developed a novel double-chain chimeric receptor Synthetic T Cell Receptor and Antigen Receptor (STAR) consisting of 2 protein modules each containing an antibody light or heavy chain variable region, the T Cell Receptor (TCR) a or b chain constant region fused to the OX-40 co-stimulatory domain, with the 2 modules linked by a self-cleaving Furin-p2A sequence that allows the modules to be proteolytically separated and reconstituted (Fig. 1A). Here, we report pre-clinical and first-in-human phase I trial results of CD19 STAR-T cell therapy for CD19+ R/R B-ALL.
Methods
Peripheral blood (PB) mononuclear cells were obtained from healthy donors and patients for the pre-clinical and clinical studies, respectively. T-cells were transduced with the STAR lentiviral vector. A leukemia xenograft mouse model was used to assess the STAR T-cell antitumor function.
For the clinical trial, from Dec. 2019 to Jun. 2020, 18 CD19+ R/R B-ALL patients (M/F 10:8) with a median age of 22.5 years (range: 6-68) were enrolled (NCT03953599). Patients received a conditioning regimen of IV fludarabine (25mg/m2/d) and cyclophosphamide (250mg/m2/d) for 3 days followed by a single STAR T-cell infusion. Once patients achieved complete remission (CR), they were given the option to proceed to consolidation allogeneic hematopoietic stem cell transplantation (allo-HSCT) or not.
Results
In preclinical studies, we found CD19 STAR T-cells to be superior to conventional CAR (BBz CAR) measured by the following parameters: 1) faster/stronger T-cell activation within 3 hours (76.67±2.621% vs 46.4±9.318%; p=0.0253); 2) higher cytokine production (4100.92±174.4 pg/ml vs 2556.78±563.39 pg/ml; p<0.05, Fig.1B) ;3) superior target killing ability (effector: target [E: T] ratio=1:1, 50.39±1.74% vs 60.85±1.52%, p<0.05. E:T ratio>1:1, p<0.01, Fig.1B); 4) robust elimination of B-ALL in a xenograft mouse model, where a lower E:T ratio was sufficient to eliminate an equal number of tumor cells (E:T ratio =1:1, STAR vs. BBz-CAR, p<0.01, Fig.1C).
In the phase I trial, the median observation time was 69 (20-180) days. The median pre-treatment bone marrow (BM) blast level was 7.0% (0.1%-86.6%). All 18 patients received a single infusion of STAR T-cells at a median dose of 1×106/kg (5×105/kg-2.5×106/kg): low dose (5×105/kg) (n=3), medium dose (1×106/kg) (n=8) and high-dose (2-2.5×106/kg) (n=7). Three early enrollees subsequently received a second consolidation infusion of STAR T-cells at 1×106/kg (n=2) and 2×106/kg (n=1). The median STAR T-cell production time was 9 (7-13) days with a transduction efficacy of 57.4% (41.0%-78.2%). Two weeks post STAR T-cell infusion, 18/18 (100%) patients achieved CR with a negative minimal residual disease (MRD) status. After a median of 57 (43-66) days following STAR T-cell therapy, 8/18 patients made a choice to pursue consolidation allo-HSCT and all have remained in CR after a median follow-up of 110 (75-180) days. Of the 10 patients who did not undergo allo-HSCT, 1 relapsed on day 58 and died from relapse on day 63. This patient had a pre-CAR T-cell BM blast level of 86.6% with central nervous system leukemia. Another patient became MRD-positive with 0.09% blasts on day 30 per flow cytometry (FCM). The other 8 patients have remained in CR.
Despite the achievement of a high CR rate, cytokine release syndrome (CRS) occurred only in 10/18 (55.6%) patients with 8 Grade I, and 2 Grade II CRS. Two patients developed Grade III neurotoxicity.
After STAR T-cell infusion, CD19 STAR T-cells in PB were followed by qPCR and FCM. We saw high in vivo proliferation and persistence regardless of the infusion dose. The median peak level was reached on day 8.5 (day 4-10) with 4.9×104 (0.104-175×104) copy number/ug PB genomic DNA detectable at 6 months.
Conclusion
This study demonstrates the superiority of STAR T-cells compared to conventional CAR T-cells in terms of signaling capacity, cytokine production capability and anti-tumor potency in an animal model. The Phase I first-in-human study demonstrated technical feasibility, clinical safety and efficacy of STAR-T in treating CD19+ R/R B-ALL. A high CR could be achieved on day 14 with low toxicity. Longer-term observation of these patients and studies of larger patient cohorts are warranted.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal